


Removal of a DEA Training Requirement Would Eliminate Treatment Barriers for OUD Providers
WASHINGTON — The House Committee on Energy and Commerce recently voted to advance provisions of two bills which would eliminate special DEA licensing and expand baseline education for treatment providers who prescribe buprenorphine — a medication approved by the Food and Drug Administration to treat those with opioid use disorder.
“There were a lot of questions around why this special licensing exists…[many treatment providers] actually think this is a pretty big barrier as a multidimensional issue relating to patient access,” said Dr. Shawn Ryan, co-founder, president and chief medical officer of Brightview Health, during a phone call with The Well News.
The special licensing in question is known as the data waiver 2000, which was established through the Drug Addiction Treatment Act of 2000, and the SUPPORT Act of 2018, to expand medication-assisted treatment using buprenorphine to additional practitioners in various settings.
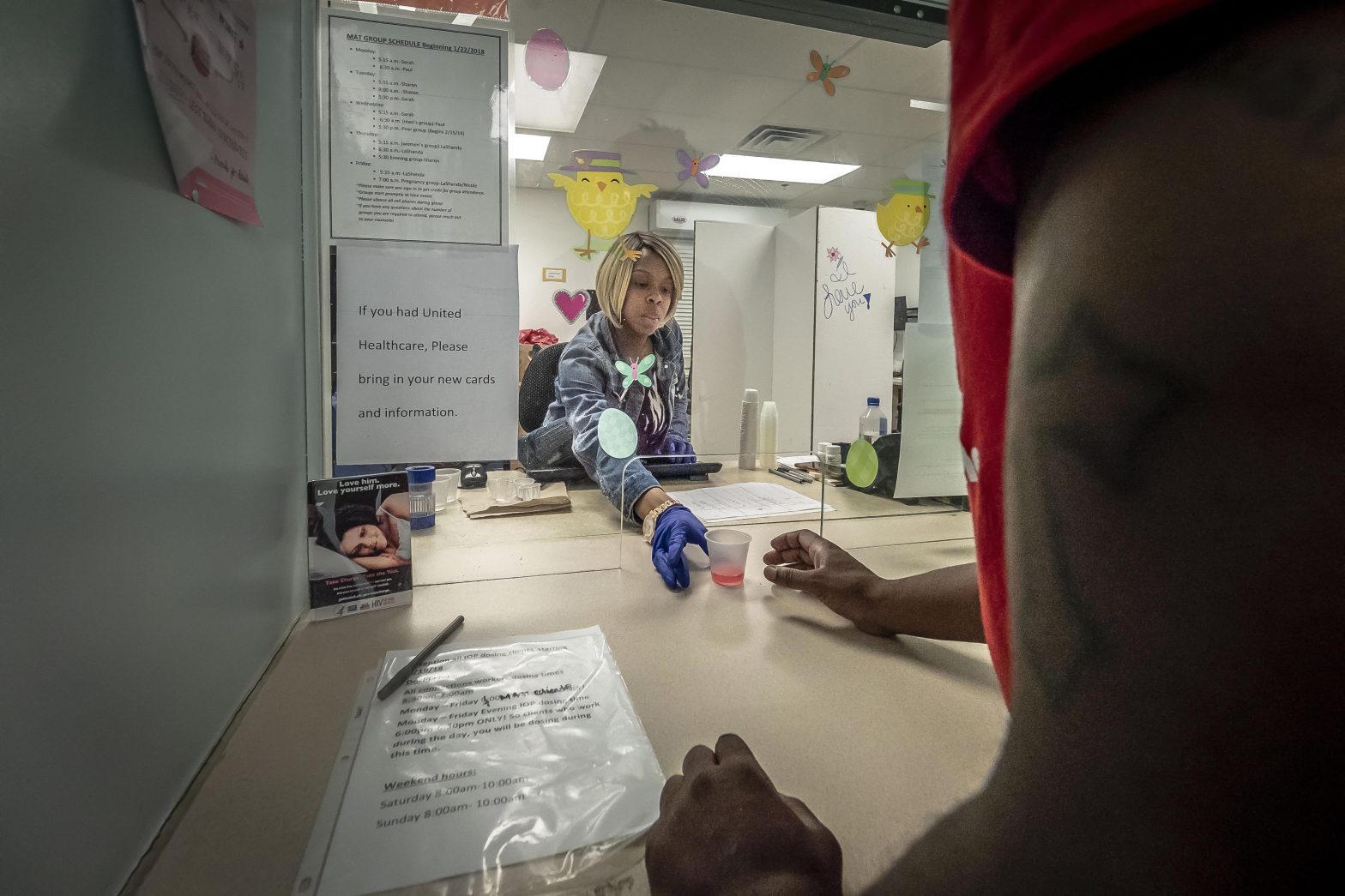
Under the requirement, to administer, dispense and prescribe buprenorphine, a practitioner must receive the DEA waiver through an eight-hour training which is specific to buprenorphine, and abide by practice guidance that limits providers to treating up to no more than 100 patients at any one time.
The Mainstreaming Addiction Treatment Act, H.R. 1384, known as the MAT Act, would eliminate the requirement that health care practitioners apply for this separate waiver through the DEA to prescribe buprenorphine for OUD treatment.
“There are little to no licensing requirements like this in medicine,” said Ryan.
“This specific license is a barrier to patient access, but we don’t want to not require some education for addiction for providers who are willing to prescribe buprenorphine,” continued Ryan.
Instead of needing to obtain the DEA waiver, the Medication Access and Training Expansion Act, H.R. 2067, known as the MATE Act , would ensure that providers have a baseline knowledge of how to treat patients with substance use disorder from accredited organizations or an accredited health professional school or residency program.
The U.S. Senate is currently considering companion pieces for both the MATE and MAT Acts.
“Is this medication so dangerous you need a special license to prescribe it? No. Is it a possible barrier to access for patients? Yes. Let’s say your primary care provider in a small town is busy seeing 40-50 patients a day. They would have to take eight hours of their time to get this special education, and it’s a very specific education to the medication,” said Ryan.
Ryan said that for the other two FDA-approved medications used to treat opioid use disorders, buprenorphine is the only one which requires this special licensing waiver.
“Buprenorphine is by and large a bit safer than methadone,” said Ryan.
The MAT and MATE legislation hit the House floor just as U.S. drug overdose deaths topped 100,000 for the first time in 2021, a 15% increase over the previous year, according to data from the Centers for Disease Control and Prevention that was released on May 11.
The National Institutes of Health published findings in 2018 that compared to those not receiving medication assisted treatment, opioid overdose deaths decreased by 38% for those receiving buprenorphine over the 12-month follow-up period.
Ryan said there are a few other barriers which the MAT Act is trying to address, such as the difficulty of having to track the number of patients that a practitioner with this special license can prescribe to in a single day.
“You have to track and maintain information on these patients specifically. So, on top of all the regular mountain of paperwork you have to do on each patient, you have to keep track of this, and the DEA does audits to make sure they have those records,” said Ryan.
“We have full time staff that do nothing but medication tracking data… there’s never been a great reason for it. Our prescribing record already has the record for the electronic prescription… and the pharmacy has it documented when they are given the medication. It’s redundant paperwork,” said Ryan.
The MAT Act would remove these limits and barriers and tracking mechanisms by lifting the requirement for DEA waiver.
“The theory here is that medical providers can, and should, be able to self-regulate how many patients they can see,” said Ryan.
Alexa can be reached at [email protected]


















